A smart technique for Maxillomandibular fixation
ABSTRACT: Numerous methods have been described for the achievement of intermaxillary fixation in the treatment of the maxillomandibular fracture. Conventional methods like Erich arch bars, eyelet wires, IMF screws are currently the most common methods for achieving intermaxillary fixation, however, they have their own disadvantages such as the risk of penetrating injury, increased surgical time, trauma to periodontium etc. This case report presents a new alternative method that can overcome the disadvantages of conventional methods.
INTRODUCTION: Maxillomandibularfixation(MMF) is a basic and fundamental principal in the managment and treatment of maxillofacial trauma. MMF serves as a cornerstone of maxillofacial reconstruction, providing a stable base from which facial form and function can be restored.[1] Risk of penetrating injury to the surgeon that subsequently increase the risk of blood borne pathogen transmission from percutaneous injuries, increase surgical time, trauma to periodontium, compromised oral hygiene, movement of teeth in lateral and extrusive direction are all shortcomings of traditional arch bars.[2,3,4,5,6] Loosening of screw and disturbance of occlusal stability after few days of placement often limit the application of IMF screw.
In the perusal of finding an alternate method of application of arch bar that can overcome maximum disadvantages and also improve clinician’s and patient’s acceptance at the satisfactory level.
CASE REPORT : A 24 years male patient was referred to Department of Oral And Maxillofacial Surgery in K.D.Dental College and Hospital, Mathura (UP) on March,2018. The chief complaint was pain, swelling and inability to chew after a road traffic accident, one day before. On examination, a laceration on lower lip, deviation of mandible to right side and tenderness in lower chin and right condylar region were noticed. Intraoralystep deformity was palpated in left parasymphysis region, tenderness was present in left parasymphysis, symphysis and right condylar region. OPG showed radiolucent line extend obliquely from left lower lateral incisior to inferior border of mandible and right condyle shift mesially. These findings indicated a possible left parasymphysis and right condylar fracture.
Under local anaesthesia the new maxillary and mandibular arch bar (MODIFIED ARCH BAR)was placed individually and fixed with the interlocking screw with capstan style head. In each arch three 2 mm diameter and 6mm length screw was placed in the attached gingiva. Two screws were placed bilaterally posteriorly and one was placed centrally under copious normal saline irrigation. After reduction of fracture intermaxillary fixation was done with 26 gauze wire followed by ORIF. Patient was kept on a course of antibiotics and analgesics, and advised to take liquid diet and to use betadinemouthwash.Regular follow-up was done for 24 hours, 3days and at weekly intervals upto two weeks. After two weeks IMF with maxillary and mandibular arch bar was released and patient recalled for 24 hours, 3days and at weekly intervals upto 1 month.
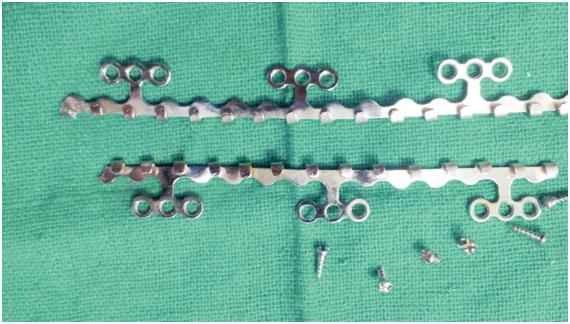
MODIFIED ARCH BAR WITH CAPSTAN STYLE
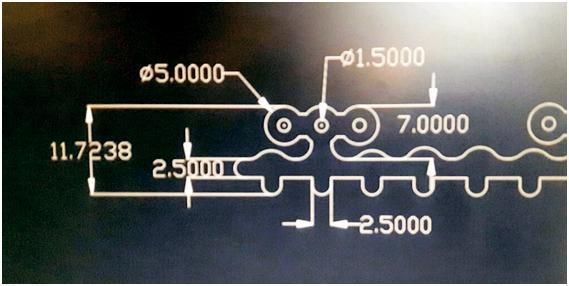
SCHEMATIC PICTURE OF MODIFIED ARCH BAR

OPG VIEW OF MODIFIED ARCH BAR
RESULT:
- Time taken for the procedure was within 20 -25mins
- Incidence of gloves injury was not reported.
- In pulp test left lower lateral incisor which was in fracture line gave delayed response immediately after removal of arch bar. Rest of teeth gave positive vitality test both post-operatively and pre-operatively.
- Stability was adequate during the placement and removal.
- Oral hygiene index was good during treatment and at the day of removal.
- Ease of placement and good patient acceptance.
DISCUSSION: The goals of closed reduction– fracture reduction, stabilization of bone and achievement of proper dental occlusion were fulfilled completely by the smart technique. As units of three loops extend from each segment of arch bar, screws can be placed in any one of the three holes of each unit to bypass the fracture line and the roots of teeth. Screws with capstan style head are also important as it allows the wires and elastics to be held away from the gingival tissue.[7,8]
One complication associated with the screws was that the screw heads became embedded in the soft tissue over a period of time and during removal necessitated the use of stab incision under local anesthesia for exposure.[9,10]
CONCLUSION : IMF with “MODIFIED ARCH BAR” is more efficacious compared to conventional methods. It improve surgeon’s and patient’s acceptance to a satisfactory level. Considering the result we conclude that “MODIFIED ARCH BAR” provide an effective alternative to traditional arch bar techniques for the treatment of maxillomandiular fracture. Further studies with large sample group should be taken up to study this new technique.
CONFLICT OF INTEREST: We have no conflicts of interest.
ETHICS STATEMENT/CONFIRMATION OF PATIENT’S PERMISSION: The study has been approved by the ethics review board of the institution. Written informed consent was obtained from the patient.
REFERENCES
- Coletti DP, Salama A, Caccamese JF Jr. Application of intermaxillary fixation screws in maxillofacial trauma. J Oral MaxillofacSurg 2007;65:1746-50.
- Nandini GD, Balakrishna R, Rao J. Self tapping screws vs Erich arch bar for intermaxillary fixation: A comparative clinical study in the treatment of mandibular fractures. J Maxillofac Oral Surg 2011;10:127-31.
- Falci SG, Douglas de Oliveira DW, Stella PEM, et al. Is the Erich arch bar the best intermaxillary fixation method in maxillofacial fractures? A systematic review of Med Oral Patol Oral CirugiaBucal 2015;20:e494-9
- Nilesh K, Karandikar S. IMF screws as an Alternative to arch bar Fixation in the management of mandibular fracture.Int J Dent Clin 2011;3:82–3.
- Chhabra N, Chhabra S, Thapar D. Evaluation of two different methods of arch bar application: a comparative prospective study. J Maxillofac Oral Surg. 2015;14(2):432–40.
- Lone P, Singh M, Salgotra V, Johar H. Role of oral prophylaxis with the use of Erich arch bars: A randomized controlled Trial. Int J Sci Stud 2015; 3(7): 18-22
- Qureshi AA, Reddy UK, Warad NM, et al. Intermaxillary fixation screws versus Erich arch bars in mandibularfractures: a comparative study and review of literature.Ann MaxillofacSurg2016;6:25–30.
- Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. Br J Oral MaxillofacSurg 2002;40:241-43.
- Lateef AT, Ismael KW, Mohnsen SS. Evaluation of Stainless Steel Intermaxillary Fixation Screws in Treatment of Favorable Mandibular Fractures.J BaghColl Dentistry 2017; 29(2):83-89.
- Rai A, Datarkar A, Borle RM: Are maxillomandibular fixation screws a better option than Erich arch bars in achieving maxillomandibular fixation? randomized clinical study. J Oral MaxillofacSurg 2011;69:3015-17.
CORRESPONDENCE AUTHOR: Dr. Soumendu Karak


0 Comments